
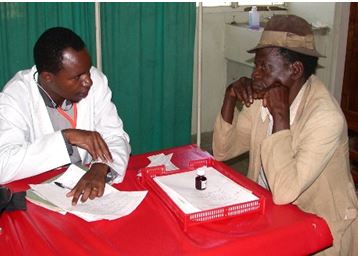
He stands, bent, outside the front of the house, the two steps up to the door being too far to lift himself leaning hard on the old stick, cloth padding the top as a cane or maybe a crutch. I step down to greet him, “Jambo,” (how are you) and to wish him “Salama,” (peace). He holds up his hands to show me the stumps of his fingers. Leprosy. Mainly, his knee hurts. It hurts worse from having walked two days to see the visiting American doctor here in the tiny village of Magu, Tanzania, located on the shore of Lake Victoria.
I feel totally helpless, humbled that he and all the others waiting to see me are so enduring, so hopeful. I have little to offer that can help leprosy or severe osteoarthritis. Bad marriages, not so much, either. Malaria, yes.
The school I am visiting used to be a hospital. It is located where Henry Morton Stanley embarked across Lake Victoria on his way to find, on November 10, 1871, the famous British medical missionary, David Livingstone (remember: “Dr. Livingstone, I presume?”). I have set up to see patients in a spare bedroom of the house in which the dean of the school raised his family.
Most medical care in the village is provided by Henry, a physician assistant who is much loved by the community because he is competent and obviously cares. Many other providers are not so competent and caring and do not stay long. Henry sees a hundred patients a day. They line up on benches: quiet, waiting, pregnant, hurting, feverish, sad. They feel better knowing Henry cares about them and sometimes because he can help them with medicine. Henry would later come to Utah for six months to learn in our physician assistant program and eventually, after overcoming many barriers, he will attend medical school in Tanzania.
The first patient I see with Henry is a teenager with night blindness. He has vitamin A deficiency. There have been no vegetables available during the drought.
Another youngster, maybe 8 years old, lies oh-so-still and quiet, supine on the exam table. The mountain rising from his belly is his spleen. Every child we see has a big spleen from malaria.
Another has a fever, cough, and, in a precise pattern, rows of small cuts on the side of his chest. Treatment from the indigenous healer for pneumonia. It didn’t work so the boy’s mother brought him to see Henry, who gave him penicillin.
I see lots of patients with back pain. They look at me like I am crazy when I suggest “good back mechanics,” and tell them to “lift with your legs,” but they are grateful for ibuprofen or acetaminophen.

So what does this have to do with family medicine in the United States? Three points of wisdom I had heard before were highlighted by the sharpness of life and health in Tanzania. We may have more stuff–more tools, more tests, more medicine, more spider webs of complex organizations, practices, teams, insurance companies, electronic medical records and even politics–but the essence of what it means to be a doctor, what it means to provide health care, becomes clearer in settings where the external things are stripped away and we are left with our hands, eyes, ears, knowledge, compassion, and a few tools to minister to our fellow human beings who may be sick, suffering, and worried. In Tanzania, I was reminded that as family physicians it is our privilege to:
- Care, always
As Francis Peabody famously said in 1927:
“The treatment of a disease may be entirely impersonal; the care of a patient must be completely personal. The significance of the intimate personal relationship between physician and patient cannot be too strongly emphasized, for in an extraordinarily large number of cases both diagnosis and treatment are directly dependent on it…The good physician knows his (or her) patients through and through, and [t]his knowledge is bought dearly. Time, sympathy and understanding must be lavishly dispensed, but the reward is to be found in that personal bond which forms the greatest satisfaction of the practice of medicine. One of the essential qualities of the clinician is interest in humanity, for the secret of the care of the patient is in caring for the patient.” (JAMA. 1927;88(12):877-882).
More recently, Marc Harrison, MD, a pediatric intensivist and now CEO of Intermountain Healthcare said it this way:
“There is perhaps nowhere else that calls out quite so clearly for a completely judgment-free atmosphere as a hospital exam room or doctor’s office…When it comes to healing, there is no room for anything but love.” (Salt Lake Tribune, August 13, 2017).
- Cure, sometimes
Hippocrates said, “Cure sometimes, treat often, comfort always.” It seems simple to say, yet difficult to live in practice, but we must always maintain commitment to truth in science. I was so very grateful in Tanzania to be able to offer penicillin instead of magic. I would much rather practice today when we wield unbelievably powerful tools of diagnosis and treatment not available even when I finished medical school, but I am also aware that science bridges beyond biology, medical diagnosis, and treatment.
Tuberculosis disease was in decline before the discovery of antibiotics against M. tuberculosis. People really do get better from the placebo effect. Environment, behavior, poverty, and lack of education kills people more than medicine saves. Your zip code is likely more important in determining your life expectancy than is your genetic code. Our infatuation with technology has distracted us from using effective treatments for prevention. The American medical business model invests heavily in intensive care to rescue people from complications of problems that would never occur if we invested in prevention and in solving the problems that arise from social determinants of health.
True science studies molecules and mechanisms of disease, but it also reaches beyond reductionism to understand context, community, and whole persons in all their puzzling complexities.
- Laugh, often
People in rural Tanzania take time for relationships. They take time for people and for each other. You do not pass someone walking the other way on the village path. Instead, you stop, talk, console, and laugh, really laugh. No matter the burdens, shared laughter helps lighten each person’s load.
Being with the strong people of a distant and different culture, this American doctor was reminded of the enduring truth of what matters. It is our great privilege to offer love via the tools we have available – both succor and science – to uplift and encourage those we encounter, wherever we find them along our paths.

Michael K. Magill, M.D., has served for 10 years as Executive Medical Director of the University of Utah Hospitals and Clinics/Community Physician Group, a multidisciplinary medical practice located in 10 sites in the Salt Lake City metropolitan area. He served as Department Chair for the Department of Family and Preventive Medicine for over a decade, and now serves as AHEC Director and works in clinics as a family medicine doctor several times throughout the week.
