by Joe Novak, MD

I love a good graph. An undergrad degree in physics drilled into me that the graph is one of the best tools to convey complex information quickly (and also one of the best tools to take up space in lab reports with a minimum page requirement).
A graph that I’ve found myself thinking about (and drawing) a lot lately shows “Age” on the X axis and “Quality of Life” on the Y axis.

(To be clear, I heard of this from a podcast featuring Peter Attia, which was in turn recommended to me by a co-resident, Rich Wolferz).
As a family medicine physician, I take care of patients who reside at pretty much every point on that graph. An average family doctor’s patient population might look like this:

My concern isn’t where any one patient is on this graph relative to another. Instead, my goal is to keep their quality of life as high as possible for as long as possible. I think most people would agree that they want their “graph” look like this:
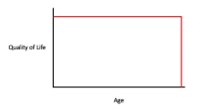
rather than this:
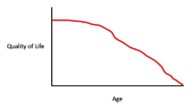
Bringing that framework to a visit helps provoke a few important questions:
- Where does a person feel like they fall on this graph?
- Why aren’t they higher on the Y axis? What’s keeping them from being higher?
- How can we keep that quality of life as high as possible for as long as possible?
Certainly, there is a role for diagnosing diseases and prescribing medications in helping answer these questions. For the majority of people, though, the role of medicine as an institution is minimal in comparison with everything else going on in their life.
Some things have a pretty clear impact on that graph. I have a hard time advocating for cigarettes as having any role in anyone’s life. But a donut? That’s harder to quantify – how does one balance the joy of eating a donut against longevity?
What about exercise? Clearly, physical activity is a crucial part of keeping peoples’ quality of life high and their lifespan long. But some people hate going to the gym, hate the guilt they feel when they don’t, and as a result may avoid physical activity altogether. How do we accommodate that? How do we help the “exercise”-averse maintain their ability to–later in life–care for themselves, pick up their grandkids, stand up out of a chair without help?
I don’t have the answers for all (or maybe even most) of these questions, but feel that it’s important ask them, and to be a resource for patients as they grapple with them.

Dr. Novak is from Saint Louis Park, MN. He completed his undergraduate education at Luther College before going to the University of Minnesota for his medical degree. His medical interests include medical education, behavioral health, inpatient medicine, quality improvement, and preventative medicine. In his free time, he enjoys mountain biking, rock climbing, skiing, cooking (especially baking bread), playing piano and guitar, and reading. He chose the University of Utah because it is a community-based program with university resources that allow its residents to shape their experience to be perfect for them. Also, it has wonderful faculty and residents, and is located in a beautiful part of the country!
